
Shanice Hastings
Dr. Licastro
English 381. Sec 01
5 May 2017
The Future Book for the Future Einstein: A Proposal
In researching the many different techniques and learning styles for children with autism, it is clear that there is currently no one universal form of treatment. According to Prizant in The SCERTS MODEL, the goal is to provide an approach that enhances socioemotional abilities, communication skills, and transactional support to both children on the autism spectrum, and their families (296). This model, like many before it, is an attempt to combine “child-centered” and “parent-centered” practices, while using an ABA approach as a base or foundation (ABA is a behavioral learning approach with A1 as baseline, B as treatment, and A2 as the extinction phase). Due to the inconstancy in technology and literature, I am proposing a tool in the form of a virtual reality book/ software. The purpose of the book is to help children with autism transition into treatment and new social environments. All while promoting growth and positive adaptive behaviors.
In the Journal of Positive Behavior Interventions, Schreibman describes the challenges children with autism face when transitioning into a new environment, or when learning a new activity (3). Although the transition phase may be scaring and overwhelming, it is important and inevitable in treatment. It is likely to see behaviors worsen during this phase. The child may become more aggressive, or engage in new behaviors such as self injury (SIB) (Schreibman, 3). Studies have shown positive implications of instructional video models as a learning tool to assists with basic living skills (Shipley-Benamou, 166). However, a program that assists with treatment, academics, and transitioning phases, all in one, does not exist at the current time.
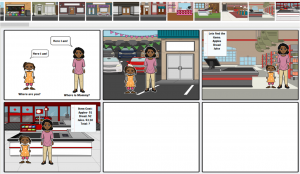
The program will simulate a learning environment through a virtual reality children’s book. The book will encompass academic and skill set education, in addition to transitional treatment and assistance. The program will also monitor progress. The virtual reality book will consist of story lines and adjustable settings within the program that can be accessed by the therapist. Instead of illustrations on a page, the child is actually in the book, interacting with characters and objects. For example, the prototype I created is called, “My First Trip to the Grocery Store.” There will be two versions of the story. The beginner version is a simple cartoon simulation of a grocery store, and the advanced version is a 3D simulation of the same thing. Depending on the child’s level of interaction he/ she will be allowed to create his/ her own avatar, or character in the book. Another great feature of this program is that it will allow for multi-players. This way, the parent has the opportunity to interact with the child. As stated in the introduction, combining child and family-centered therapy has been a challenge in the approach and sustainability of treatment (Prizant, 296). Therefore, it is imperative to include the parent and family in the virtual reality experience. The family will acquire the tools needed to learn how to respond to behaviors, how to implement directives and treatment in absence of a therapist, as well as when to give positive reinforcements. For this reason, the directives given to the parent player will be different from directives given to the child player. For instance, in the setting of a grocery store the child can be directed to find the apples. If the child is having trouble finding the apples, the parent will be directed to offer assistance. The parent will be told what to say, by the program or the therapist, who will act as an observer. The main idea is for the parent will to interact with their child, learn what works opposed to what does not work, and practice them in a safe environment. As a result, both child and parent will feel confident in natural settings because they both have conquered the challenge of being in a new environment.
In conceptualizing the mechanics of the program, there are multiple challenges to be address. To assess whether or not the child is paying attention to directives we will incorporate an eye tracking device on the inner lens of the VR goggles. This device will track where the child is looking and when, at all times. The lens will connect to the main board of the program in order to send a signal that says the child is looking in the correct direction, or not. Then, the program will know to show arrow marks to catch the child’s attention, or highlight the mom character for help. The child will be directed to explore items by using his/ her hands to tap, or motion over them. This brings me to another feature of the VR goggles. If the child is to interact with the story through touch and motion, I would create Bluetooth signaled devices that will be attach to the finger tips. Another challenge will be controlling auditory stimuli. It is common for children on the autism spectrum to struggle with sensory overload (American Psychiatric Association). To prevent this issue, the goggles will need specific and specially made earphones that will block outside noise. The sound in the program will be adjustable by the therapist. Sensory stimuli will be introduced when the child is ready and as the therapist sees fit. For the purposes of this specific prototype, the setting will not include any additional auditory stimuli besides a monotone voice, giving directions. The idea is to perfect a prototype by testing and troubleshooting issues that may arise in the creation process. The main goal is to have a program flexible enough to customize to each individual child, and where they currently are in their learning and coping process. I would like for this device to be usable for children across the spectrum, including those with severe behaviors. The goggles will be durable enough to withstand any possible physical damage, yet light weight enough to manipulate for a child who may wear protective gear.
If you imagine what such book would look like, I would describe the concept of program one as a cartoon simulation (beginners), and program two, more life-like (advanced). The beginners program will start with a series of levels from 0-10. The child will move up in levels by following directions and earning stars, points, or coins. The goggles will detect movement and differentiate between positive behavior and negative behavior such as aggressions and self injury. For example, James is a beginner. James engages in moderate to severe SIB. One of his SIBs is skin picking. With the connection between the VR goggles and the Bluetooth fingertip reader, the program will detect whenever James picks at any part of the body and deduct a point or coin. James may earn points by correctly answering questions, or not engaging in SIB for a period of time. Of course, the therapist will be able to manipulate this feature from their end. Although, the therapist is a player only to observe, he/ she will also adjust settings to custom fit the child and his/ her needs. The program will collect and save data for each trial. This feature allows the therapist to compare his/ her observations to the data collected by the program. Since this program is intended to be an effective learning tool, it may be used for any particular thing the child is struggling with. It is not meant to be forced upon the child to use, but slowly introduced. This may mean having the child see it, then take it away. Then, have the child feel it for a moment then take it away. Next, have the child wear it for a few minutes at a time and take it away. This, too, is a new experience itself and should be introduced in moderation. Studies have shown positive feedback in social communication when visual stimuli was used in treatment of children with autism. Thiemann and Goldstein found that 10 minutes of social interaction and 10 minutes of self evaluation using video feedback increased desired social behaviors and communicative skills (426).
This new technology is intended to give children with autism an alternative way to learn. This non-traditional approach is necessary when accommodating children with a different set of needs. In coping with their disorder, I hope this program will help children take what they have learned and apply it to real life scenarios, while decreasing problem behaviors and increasing pro social skills. Although the original program is geared toward children with autism, it is not limited to one disorder. Eventually, there will be a variety of different stories written by the best authors of children’s books. I hope that this book will give children and their families a sense of hope for the future, and unlock the genius potential behind the unrecognized Einstein.
Work Cited
American Psychiatric Association, and American Psychiatric Association. “DSM-5 Task Force.(2013).” Diagnostic and statistical manual of mental disorders: DSM-5™. Arlington, VA: American Psychiatric Publishing.
Prizant, Barry M., et al. “The SCERTS Model: A transactional, family‐centered approach to enhancing communication and socioemotional abilities of children with autism spectrum disorder.” Infants & Young Children 16.4 (2003): 296-316.
Schreibman, Laura, Christina Whalen, and Aubyn C. Stahmer. “The use of video priming to reduce disruptive transition behavior in children with autism.”Journal of positive behavior interventions 2.1 (2000): 3-11.
Shipley-Benamou, Robin, John R. Lutzker, and Mitchell Taubman. “Teaching daily living skills to children with autism through instructional video modeling.”Journal of Positive Behavior Interventions 4.3 (2002): 166-177.
Thiemann, Kathy S., and Howard Goldstein. “Social stories, written text cues, and video feedback: Effects on social communication of children with autism.” Journal of applied behavior analysis 34.4 (2001): 425-446.