
 https://docs.google.com/document/d/1S_tSRZYlAdClSF52xO3dK52Ae7capgttajqetJWiX9k/edit
https://docs.google.com/document/d/1S_tSRZYlAdClSF52xO3dK52Ae7capgttajqetJWiX9k/edit
Link to presentation: https://docs.google.com/presentation/d/1Ofvn19BFc4OTb7nbAx3Q0j5l_Sbv-RwSFuBQsw3E5BA/edit#slide=id.p

Above is the story board for the Neonatal Abstinence Virtual Reality.
Neonatal Abstinence Proposal
David Grant
Monica Patel
Lauren Lloyd
Gregory Leonard
Andrea Ventura
Introduction:
Neonatal Abstinence Syndrome is a group of problems that occur in a newborn who was exposed to addictive opiate drugs while in the mother’s womb (medlineplus). As a result, nurses must be trained in order to have skills that prepare them for this certain task. Virtual Reality can not only train nurses, in an advanced timing. In addition, the nurses are able to experience a real life situation in caring for not only an infant but also the mother when dealing with NAS. The genre of this virtual reality program is realistic fiction, and educational, so that individuals can observe the reality of Neonatal Abstinence Syndrome. The purpose of this virtual reality program is to educate about the dangers of drug use on babies via the simulation of Neonatal Abstinence Syndrome.
Commitment:
As a Virtual reality company, we are committed to researching and implementing the latest VR technologies into our products and developing the best quality experiences. Our prototype technology will be implemented into learning hospitals to optimize the learning methods used by nurses. The success of the product will lead to the more permanent application of the learning technology into more hospitals across the country and eventually globally. As technology expands and becomes more advanced, we will adapt our current technologies to become improved and up to date with the latest applications of VR.
We are determined to making VR a reality in the teaching world. It has been shown that basic skills learned and practiced using VR have been successfully integrated into the real working medical field. As we start to integrate this one learning experience into the teaching world we will use our research to come out with more learning opportunities and different VR experiences that will continue to help the education of Nurses around the world.
Our company is initially applying this technology for the learning purpose of nursing students. This is a great first step, however; we realize that the medical field is not just limited to nurses. It is our hope that in the years to come, our technology will expand and we will be able to apply our VR experience to more learning areas in the medical field.
Long Term Vision:
Technology is forever evolving and is constantly being incorporated into our daily lives. The long-term goal of our project is to incorporate this VR program into the fast-paced and sensitive work environment of hospitals. Our society has lost touch of empathy and sympathy towards others. Nurses that take care of such patients need the skills to properly handle these sensitive situations without judgment towards the patient. Starting small with local clinics is the first step to positive change on the world.
Our project’s vision is to train new nurses and caretakers to see what it is like from the standpoint of a mother with a drug addiction. Ginger L. Arrowood wrote a journal explaining her experience at a hospital where she overheard a mother crying helplessly as her child would not stop crying. Arrowood also has a son and compare her experience stating “Our newborns are so similar – they’re both boys, with similar weights…Mine was just irritable but he is suffering from exposure to maternal drug use in utero.”. This amount of compassion does not exist in many nurses so when treating mothers with addiction, nurses can be harsh and judgemental. In Delaware, the amount of substance abuse mothers is increasing. Our VR program will ultimately be informative to the public by teaching mothers the risks and ways to prevent neonatal births. Secondly, it is our mission to pass this VR experience first hand to nurses across the country creating a more empathetic environment for these mothers.
In Conclusion, the long term objective of our project is to create a better environment for patients/mothers who are trying to keep their newborn healthy and ensure that nurses that are attending to these patients have the proper training in response to the addiction of pregnant mothers. With the help of this grant, we can be one step closer to helping millions of mothers who need help.
Implementation Strategy:
Virtual Reality for Neonatal Abstinence Syndrome requires an excessive amount of project planning. Within this planning, there are potential barriers such as cost that could either improve the project or result in failure. Making sure that the project is maintained within the budget is key in making sure that this simulation is successful. In addition, there are other barriers such as technical constraints. Using modern technology for an advanced project could delay the timing of the implementation of the project. There is also existing technology which would present as competition for VR that is focused on Neonatal syndrome. Examples of existing VR used in the medical field is Second Life which can be used for all medical students such as nurses, surgeon, physician, etc. However, regarding all the barriers there are solutions to make sure that this VR is successful. Making sure that Project Planning, management, and communication, is kept up to date so that this project does not fail.
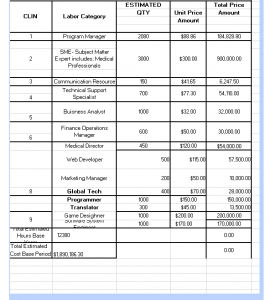
The attached Chart demonstrates the Budget for this Virtual Reality. The Budget is $7 million, as illustrated the team is well within the budget. This will result in the success of this virtual reality simulation.
Engagement – Interface:
Like most medical simulations/educational games, the interface for our VR prototype is entirely animated. This makes the prototype more interactive and allows for more development of research on the subject continues. As opposed to going back and re-filming the entire video in VR when something changes, all we have to do is go in and edit a couple of lines of code. Animation also allows for the production of the prototype to be cheaper and safer than a video.
It is important to note that the animation for this project will be as realistic as possible. There is still a certain stigma surrounding video games, often calling to mind a Super Mario game or something along those lines; rest assured that this is not the model for our game. There have been significant advances in animation technology in the last few years, and we are confident in the available resources and their ability to be used as a tool to create the best simulation possible.
In terms of controls, our prototype is fairly straightforward. Rather than follow the model of educational games like Inmind, which requires the rapid jerking of the head in a way that would likely be unsustainable for a period of time longer than about 6 minutes, our prototype would require less movement. Fitting, seeing as our simulation is largely decision-based.
This simulation can be used as a supplement for non-traditional, online nursing students that are juggling between home, work and other important commitments. As well as help improve the in-classroom experience, reducing its costs and limitations. Students that use our VR model should also be able to reinforce and strengthen concepts and knowledge learned about the Neonatal Abstinence Syndrome. Specifically for nursing students, it should be able to augment their set of skills in regards to successfully taking care of a baby with this type of syndrome.
Engagement- User Experience
The VR experience is going to not only enhance the classroom experience for a nursing student but also become an engaging tool that will heighten learning and skills needed to properly take care of a mother and baby who suffer from the neonatal abstinence syndrome. For this purpose, our VR experience will have two general options to choose from an “In Class” and an “In Mother/Infant Unit”.
If choosing the “In Class” option, the user will be able to attend class, like a regular student. By customizing an avatar that looks like them, they will go inside a room with chairs, a board, and their teacher in front of the classroom. They will be able to not only listen to the lecture but will be able to ask questions to their teacher and make comments to their classmates through a texting option available. The teacher will be able to address those questions without having to interrupt the lecture and every user attending the class will be able to see them. We want to satisfy the gamer through the learning experience not only by throwing new terms at them but allowing them to develop the course through a social environment, just like attending class in person. We will help them achieve this by allowing realistic-looking human avatars and interactions with not only the teacher but with other attendees (Johnson, 2009).
The “In Mother/Infant Unit” option is the other platform on which we are looking to develop a learning experience that is motivating and entertaining. The user will be able to immerse in the video game with their avatar, creating an identity and triggering a commitment to pursue the challenges of the game. As well, the gamer will be able to have interactions not only with the patient but also with other users of this platform, just like in the “In Class” option. We want the gamer to be able to experience real-world challenges, so information learned in the game can be applied to their nursing careers (Johnson, 2009). Thanks to the realistic-looking avatars, the user will be able to empathize and connect with the people he or she is working with and for. The decisions they make are going to influence how the game progresses, inspiring them to pursue and explore the various different ways it could go right or wrong. With the use of different levels, going from easier to expert, the gamer will not only be able to increase abilities of how to handle the neonatal abstinence syndrome but be more willing to take risks and learn the do’s and dont’s and experience first hand its consequences without hurting any real person. The game will allow single and multiplayer options, allowing the user to adventure themselves for an episode of the syndrome alone or with other users. As regular entertaining video games out there, this VR experience will also allow the gamer to not only customize their avatar but their whole nursing adventure as well (Gee, 2007). Language, skill level and length of the pregnancy in a certain level, are some examples of customization options.
The different levels found in the VR game will each target a different unit that correlates with what is being currently taught in the “In Class” platform. This means that it will follow a sense of easier, basic terms up to more complex and harder skills, terms and knowledge. Whatever is found on a certain level will be used not only to pass that level but as the game progresses, that same knowledge will have to come in handy again to solve even more complex problems found with the patient or patients (Gee, 2007). This way through engagement, repetition, identity and experience, the user will not only find the VR game entertaining but also highly educational.
Conclusion:
In conclusion in order to keep up with the changes in time, and technology you recognize that there is a need to have an alternate way of being able to educate nurses on NAS. This key benefit of this simulation is experiencing real-life scenarios in order to prepare individuals. Our VR simulation will not only help advance nurses skills but also make sure that they are able to handle any situations with mothers/infants that are dealing with Neonatal Abstinence Syndrome.
Integrity Statement: “I pledge on my honor that I have neither given nor received unauthorized assistance on this assignment/exam.
Work Cited:
Arrowood, Ginger L. “Eyes of a Mother.” Science Direct. Cross Mark, 2016. Web. 5 Dec. 2016. <http://dx.doi.org/10.1016/j.nwh.2016.08.003>.
Barthell, Jane E., and Jeanne D. Mrozek. “Neonatal Drug Withdrawl.” Clinical and Health Affair (2013): 48-50. Minnesota Medicine. Minnesota Medicine. Web. <http://eds.b.ebscohost.com/eds/detail/detail?sid=aed8c500-60ca-4b3c-bef1-b47b38b6d01f@sessionmgr107&vid=0&hid=103&bdata=JnNpdGU9ZWRzLWxpdmUmc2NvcGU9c2l0ZQ==#AN=23930471&db=mnh>.
Gee, James Paul. “GOOD VIDEO GAMES AND GOOD LEARNING.” (2007): 1-13. Web.
Johnson. “Journal For Virtual Worlds Research.” Virtual Worlds in Health Care Higher Education | Johnson | Journal For Virtual Worlds Research. N.p., 2009. Web. 08 Dec. 2016. <https://journals.tdl.org/jvwr/index.php/jvwr/article/view/699/498>.
MK, Savin, and Paul DA. “Opioid Exposed Mothers.” Public Health, Apr. 2016. Web. <https://ezproxy.stevenson.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=mnh&AN=27263243&site=eds-live&scope=site>.
“Neonatal Abstinence Syndrome: MedlinePlus Medical Encyclopedia.” MedlinePlus Medical Encyclopedia. N.p., n.d. Web. 08 Dec. 2016. <https://medlineplus.gov/ency/article/007313.htm>.